

The breast can be investigated using a few methods, which include ultrasound, X-ray (mammography), MRI and thermography. At the moment, breast ultrasound and mammography remain as the main modalities frequently used.
So how does one choose which one to go for?
Women undergoing asymptomatic screening for breast cancer should undergo mammography as the first line. This is because mammography can detect microcalcifications as seen in DCIS (ductal carcinoma in situ), an early manifestation of breast cancer. DCIS can turn into invasive cancer in up to 50% of patients within the period of 10 years.
Ultrasound on the other hand, cannot pick up microcalcifications as good as mammography.
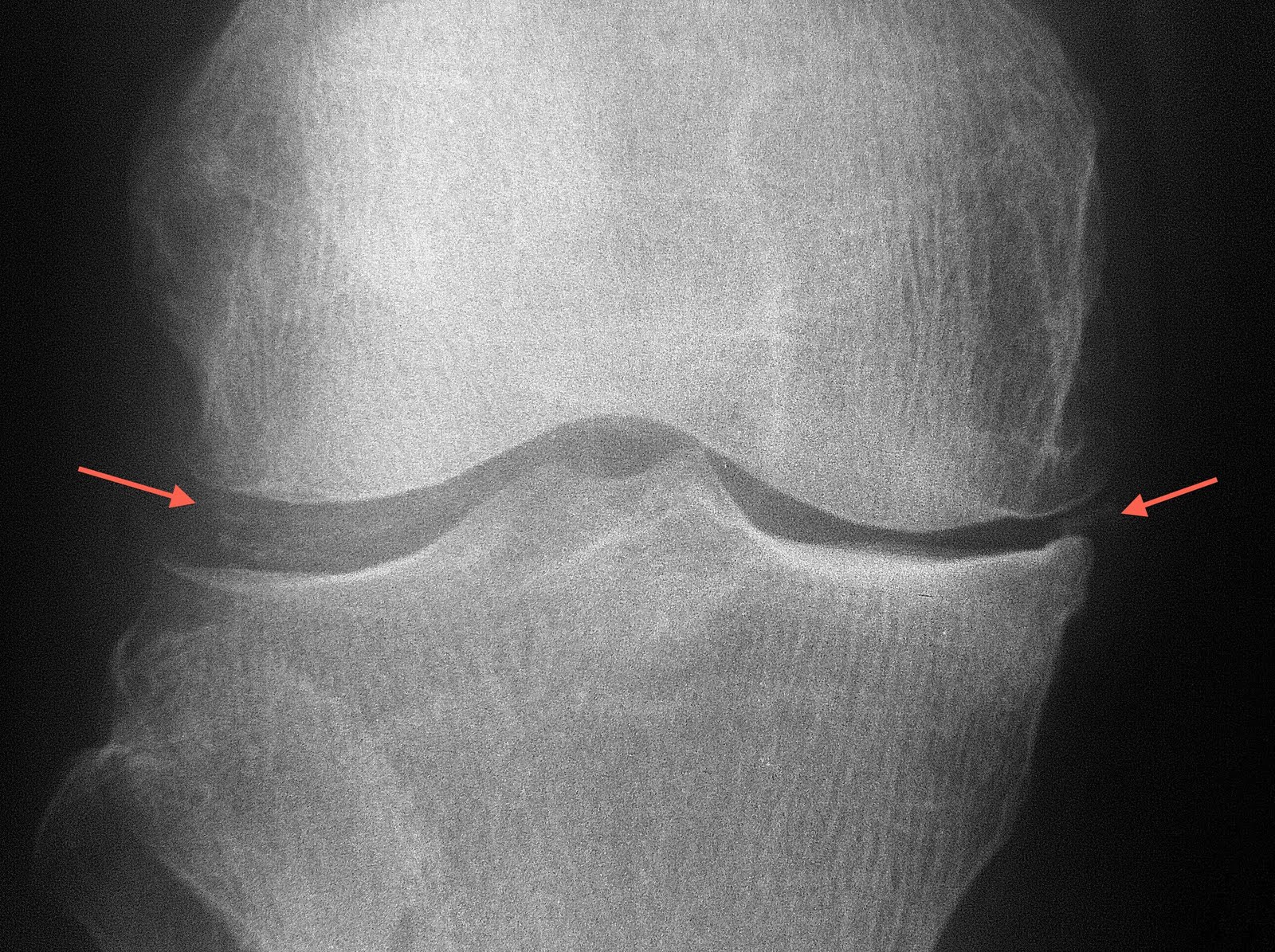
During mammography, another important finding is presence of a mass. If a mass or nodule is detected, it will be shown as a "white" shadow. Mammography can assess the margins of the lesion, the degree of 'whiteness" (density) of the lesion, presence of spicules, architectural distortion.
However, some women have very dense breasts, i.e. very thick glandular tissue. Hence the normal glandular tissue can obscure the mass lesion as both normal glandular tissue and mass lesion appear as white area on mammogram. Therefore patient with dense breasts (Bi-Rads category 3 and above) are routinely offered complimentary ultrasound to exclude mass lesion. Dense breasts do not hide the microcalcifications on mammogram, thus is not a concern for missing DCIS.

Picture on the left is a Peruru Mammography Unit which the centre currently owns and operates. It has won gold prize in Good design award in 2007 due to its ergonomic design and the patient comfort it provides.

Example of a mammogram. Arrow points at a well defined mass lesion which turns out to be a benign neoplasm (fibroadenoma)
 During one of my cycling trips, I reached the Laila Taib college building where the old Sibu airport used to be. As the skies were casting a beautiful sunset behind the college building, I stopped and attempted to capture a picture of the setting sun. When I focused at the skies, the building was dark and vice versa. Guess I need a filling light big enough to fill the college building if I were to catch the magnificent sunset as well.
During one of my cycling trips, I reached the Laila Taib college building where the old Sibu airport used to be. As the skies were casting a beautiful sunset behind the college building, I stopped and attempted to capture a picture of the setting sun. When I focused at the skies, the building was dark and vice versa. Guess I need a filling light big enough to fill the college building if I were to catch the magnificent sunset as well.















































{kind=link}