This young patient presented with pain in the region of tibial tuberosity region. He is active in school and participated in a number of sports activity.
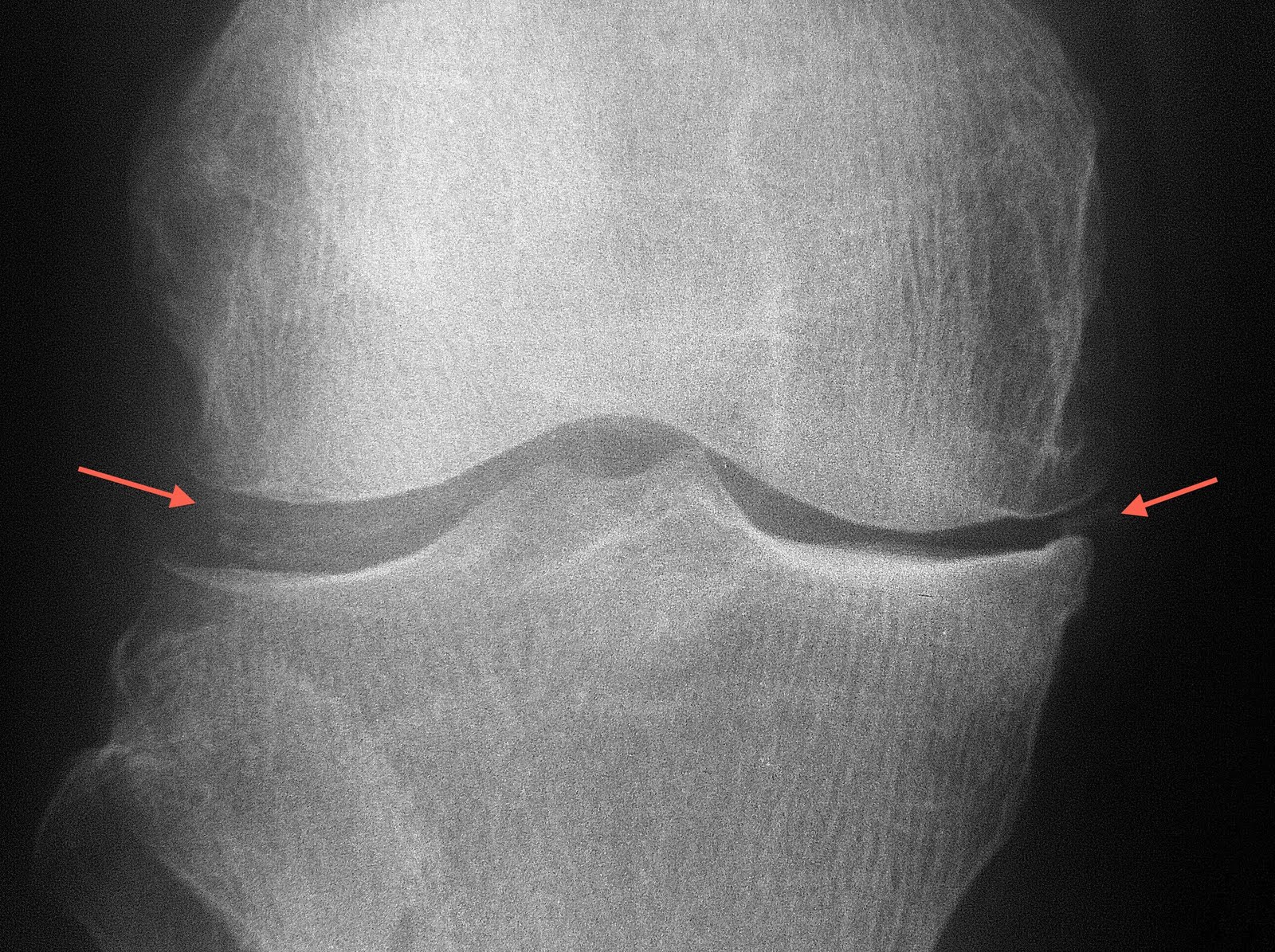
Can you spot the abnormality marked with the arrow?
The lateral knee radiograph shows separation of the ossicles from the ossification centre of the tibial tuberosity. One may also seen soft tissue thickening anterior to the tibial tuberosity.
The diagnosis is Osgood Schlatter disease. It is ne of the most common causes of knee pain in the adolescent. Consisting of pain and edema of the tibial tubercle (and hence this is an extra-articular disease), Osgood-Schlatter disease is generally a benign, self-limited knee condition associated with traction apophysitis of the tibial tubercle due to repetitive strain on the secondary ossification center of the tibial tubercle.
The aetiology of the condition is thought to be due to bone growth which is faster than soft tissue growth, resulting in muscle tendon tightness across the joint and loss of flexibility.
During periods of rapid growth, stress from contraction of the quadriceps is transmitted through the patellar tendon onto a small portion of the partially developed tibial tuberosity. This may result in a partial avulsion fracture through the ossification center. Eventually, secondary heterotopic bone formation occurs in the tendon near its insertion, producing a visible lump. Approximately 25% of patients have bilateral lesions.
Treatment is conservative with immobilization and steroid injection for symptomatic relief.
Possible complications that can follow include nonunion of bone fragment, patellar subluxation, chondromalacia, avulsion of patellar tendon, genu recurvatum.
 During one of my cycling trips, I reached the Laila Taib college building where the old Sibu airport used to be. As the skies were casting a beautiful sunset behind the college building, I stopped and attempted to capture a picture of the setting sun. When I focused at the skies, the building was dark and vice versa. Guess I need a filling light big enough to fill the college building if I were to catch the magnificent sunset as well.
During one of my cycling trips, I reached the Laila Taib college building where the old Sibu airport used to be. As the skies were casting a beautiful sunset behind the college building, I stopped and attempted to capture a picture of the setting sun. When I focused at the skies, the building was dark and vice versa. Guess I need a filling light big enough to fill the college building if I were to catch the magnificent sunset as well.